Poster Presentation The Annual Scientific Meeting of the Endocrine Society of Australia and the Society for Reproductive Biology 2014
Cryptic pulmonary lesions in ectopic ACTH syndrome (#264)
Case1. A 63-year-old woman with resistant hypertension and osteoporotic crush fractures was confirmed to have marked hypercortisolism with raised ACTH(31.3pmol/L). Repeated high-dose dexamethasone suppression tests failed to suppress cortisol. Brain MRI was inconclusive reporting possible pituitary microadenoma.
IPSS with CRH stimulation localised a central source of ACTH production to the Left(Figure1). Despite two transphenoidal hypophysectomy on two occasions she had persistent postoperative hypercortisolaemia unresponsive to ketoconazole therapy. Histopathology showed normal pituitary tissue(Figure2-A) with an incidental finding of a sphenoid mycetoma with aspergillus species.
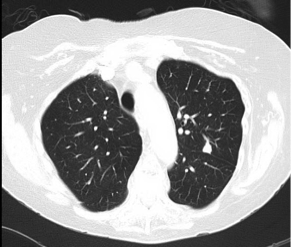
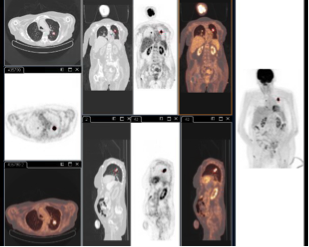
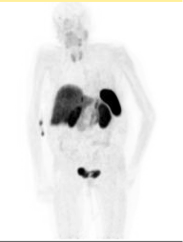
Subsequently she was discovered to have bilateral pulmonary lesions and possible liver lesions on CT/MRI. FDG-PET and Ga68-Octreotide-PET were performed: both upper lobe lung lesions demonstrated FDG-avidity but no uptake on the Ga68-Octrotide scan(Figure3-A/B/C). She underwent pulmonary core biopsy twice(initial biopsy non-diagnostic) with normal/non-malignant histopathology(Figure2-B). Repeat lung biopsy and bronchoscopic lavage culture both yielded Nocardia asteroids, for which she was successfully treated with Bactrim(sulfamethoxazole-trimethoprim).
Due to persistent symptomatic hypercortisolaemia unresponsive to adrenal blockade with high-dose ketaconazole, the patient underwent emergency bilateral adrenalectomy with successful recovery.
Figure1
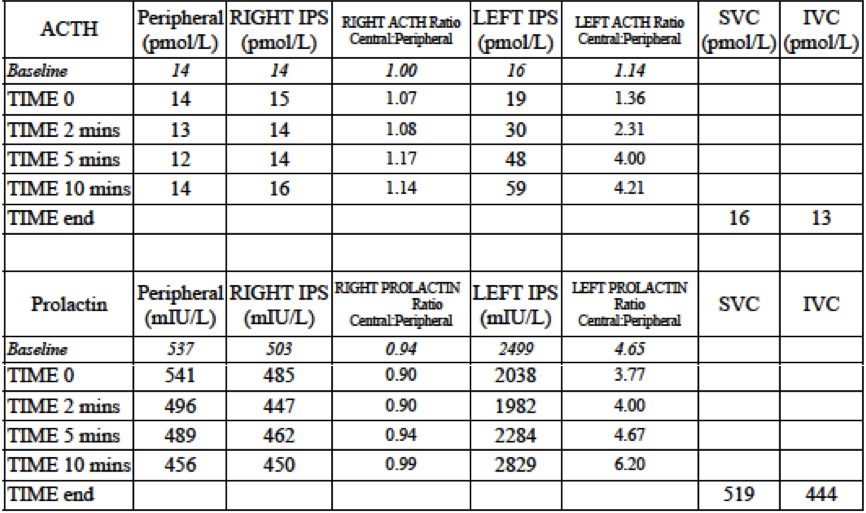
Figure2-A/B
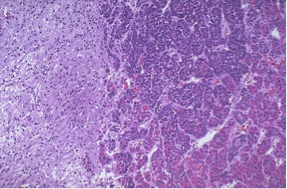
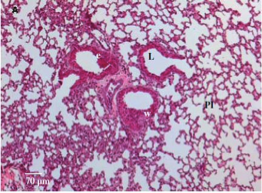
Figure3-A/B/C
Case2. A 64-year-old Caucasian male presented with erratic glycemic control with recurrent psychosis, hypokalemia, hypertension and lymphopenia. Further investigations detected cavitating lung and multiple liver lesions. PET scan showed FDG uptake in the above lesions and also in the head of pancreas and pylorus. He underwent fine need aspiration of the lung lesion and Nocardia asteroids were found.
Core biopsy of the liver lesion revealed intermediate-grade neuroendocrine tumour with ACTH-positive stain. The 24-hour urine cortisol excretion was elevated, so was serum ACTH(86.1pmol/L). He was started on ketoconazole/metyrapone and palliative chemotherapy.
Discussion: These two cases illustrate complex presentation of ectopic ACTH syndrome with a serial of diagnostic and management challenges, including severe immunosuppressive complications. We will present literature review on data of relevant results, investigational modality and currently available therapy.
- Salgado LR, Fragoso MCBV, Knoepfelmacher M, Machado MC, Domenice S, Pereira MAA and de Mendonca BB. Ectopic ACTH syndrome: our experience with 25 cases. European Journal of Endocrinology 2006; 155: 725–33.
- Stewart PM, Walker BR, Holder G, O’Halloran D and Shackleton CH. 11 beta-Hydroxysteroid dehydrogenase activity in Cushing’s syndrome: explaining the mineralocorticoid excess state of the ectopic adrenocorticotropin syndrome. Journal of Clinical Endocrinology and Metabolism 1995; 80: 3617–20.
- Isidori AM, Kaltsas GA, Pozza C, Frajese V, Newell-Price J, Reznek RH, Jenkins PJ, Monson JP, Grossman AB and Besser GM. The Ectopic Adrenocorticotropin Syndrome: Clinical Features, Diagnosis, Management, and Long-Term Follow-Up. Journal of Clinical Endocrinology and Metabolism 2006; 91: 371–7.
- Natale R, Yagoda A, Brown A, Singer C, Stover D and Bajorunas D. Combined Pneumocystis Carinii and Nocardia asteroides pneumonitis in a patient with an ACTH-producing carcinoid. Cancer1981; 47: 2933-5.
- Graham BS and Tucker WS Jr. Opportunistic Infections in Endogenous Cushing's Syndrome. Annals of Internal Medicine. 1984; 101: 334-8.
- Beinart GA, Rao RK and Hollander H. Ectopic ACTH Syndrome Resulting in Nocardiosis and Acute Respiratory Failure. Hospital Physician 2003; 39 (10): 49-51.
- Sutton BJ, Parks GE, Manavi CK, Palavecino EL and Geisinger KR. Cushing’s Syndrome and Nocardiosis Associated With a Pulmonary Carcinoid Tumor: Report of a Case and Review of the Literature. Diagnostic Cytopathology 2011; 39 (5): 359–62.
- Lindsay JR and Nieman LK. Differential diagnosis and imaging in Cushing’s syndrome. Endocrinology and Metabolism Clinics of North America 2005; 34: 403–21.
- Wind JJ, Lonser RR, Nieman LK, DeVroom HL, Chang R and Oldfield EH. The Lateralization Accuracy of Inferior Petrosal Sinus Sampling in 501 Patients With Cushing's Disease. Journal of Clinical Endocrinology and Metabolism 2013; 98 (6): 2285-93.
- Ritzel K, Beuschlein F, Mickisch A, Osswald A, Schneider HJ, Schopohl J and Reincke M. Outcome of Bilateral Adrenalectomy in Cushing’s Syndrome: A Systematic Review. Journal of Clinical Endocrinology and Metabolism 2013, 98 (10): 3939–48.